

Heart failure: Pathophysiology and Diagnosis
DEFINITION
A complex clinical syndrome that results from structural or functional impairment of ventricular filling or ejection of blood, which in turn leads to the cardinal clinical symptoms of dyspnea and fatigue and signs of HF (edema and rales)
ETIOLOGY 病因學
Etiology of HF in patients with a preserved EF differs from that of patients with depressed EF, there is considerable overlap.
收縮功能正常/異常的心臟衰竭患者病因不太一樣,但重疊的原因滿多的(右圖)
In industrialized countries, CAD has become the predominant cause in men and women and is responsible for 60–75% of cases of HF.
在已開發國家,冠心症是造成心衰竭的大宗原因,占百分之六十到七十;而高血壓也不惶多讓,占百分之七十五(兩者常常有重疊);當然,糖尿病也貢獻了很大一部分(畢竟血糖不好血管也不會好)。
Hypertension contributes to the development of HF in 75% of patients,
including most patients with CAD. Both CAD and hypertension interact to augment the risk of HF, as does diabetes mellitus.
20–30% of the cases of HFrEF, the exact etiologic basis is not known, while a large number of cases of dilated cardiomyopathy are secondary to specific genetic defects
在收縮功能有明顯異常的病例當中,有百分之二十到三十的患者原因不明;而擴張性心肌病變則多跟基因有關(OS: 好倒楣阿)

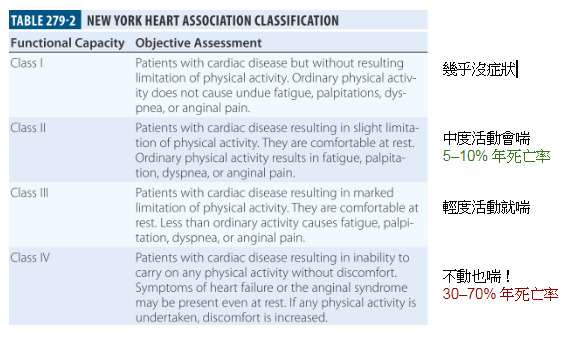
PROGNOSIS
Recent advances in the evaluation and management of HF, the development of symptomatic HF still carries a poor prognosis.
Community-based studies indicate that
30–40% die within 1 year of diagnosis
60–70% die within 5 years
mainly from worsening HF or as a sudden event (eg. ventricular arrhythmia).
PATHOGENESIS
HF may be viewed as a progressive disorder that is initiated after an INDEX EVENT

一開始不太會有症狀,是因為人體有很多的代償機制
Although the precise reasons why patients with LV dysfunction may remain asymptomatic is not certain, one potential explanation is that a number of compensatory mechanisms become activated in the presence of cardiac injury and/or LV dysfunction to sustain and modulate LV function for a period of months to years.
Heart Failure with a Reduced Ejection Fraction HFrEF的機轉

分子生物學層面看心臟衰竭的內在機轉整理圖

Myocardial relaxation is an adenosine triphosphate (ATP) dependent process that is regulated by uptake of cytoplasmic calcium into the SR by SERCA2A and extrusion of calcium by sarcolemmal pumps (see Fig. 265e-7). Accordingly, reductions in ATP concentration, as occurs in ischemia, may interfere with these processes and lead to slowed myocardial relaxation.
心肌細胞舒張是需要 ATP 的主動運動,所以如果心肌細胞因為某些原因 —— 缺血、缺氧、受損 —— 而使得細胞內的 ATP 濃度下降,心肌細胞的舒張就會不正常(OS:就像重量訓練完伸展是要主動做的)
個人對於舒張不完全對心臟功能的影響之理解
Alternatively, if LV filling is delayed because LV compliance is reduced (e.g., from hypertrophy or fibrosis), LV filling pressures will similarly remain elevated at end diastole (see Fig. 265e-11).
如果左心室肥大或心室壁變硬導致左心室的順應性下降(想像氣球變成籃球),左心室的填充變慢(氣球還可以用吹的,籃球吹得起來?),左心室在「舒張末期」的填充壓就會上升(如前述,請記得左心室的填充很大一部分是靠心室的舒張來達成,而不是心房收縮擠下來喔)。
An increase in heart rate disproportionately shortens the time for diastolic filling, which may lead to elevated LV filling pressures, particularly in noncompliant ventricles. Elevated LV end-diastolic filling pressures result in increases in pulmonary capillary pressures, which can contribute to the dyspnea experienced by patients with diastolic dysfunction.
除了心室本身的影響,如果今天心率變快,會不成比例地縮短舒張期的填充時間(導致舒張不完全),而因為舒張會降低左心室的壓力,所以舒張不完全,會導致左心室在舒張期末的壓力上升⋯⋯


In addition to impaired myocardial relaxation, increased myocardial stiffness secondary to cardiac hypertrophy and increased myocardial collagen content may contribute to diastolic failure. Importantly, diastolic dysfunction can occur alone or in combination with systolic dysfunction in patients with HF.
因為心臟肥大(好發於慢性高血壓患者)和心肌細胞壞死後由膠原細胞取代導致變硬,都會造成心室的舒張異常。而在心臟衰竭的病人身上,舒張異常有可能獨立存在,也可能同時伴隨著收縮異常。